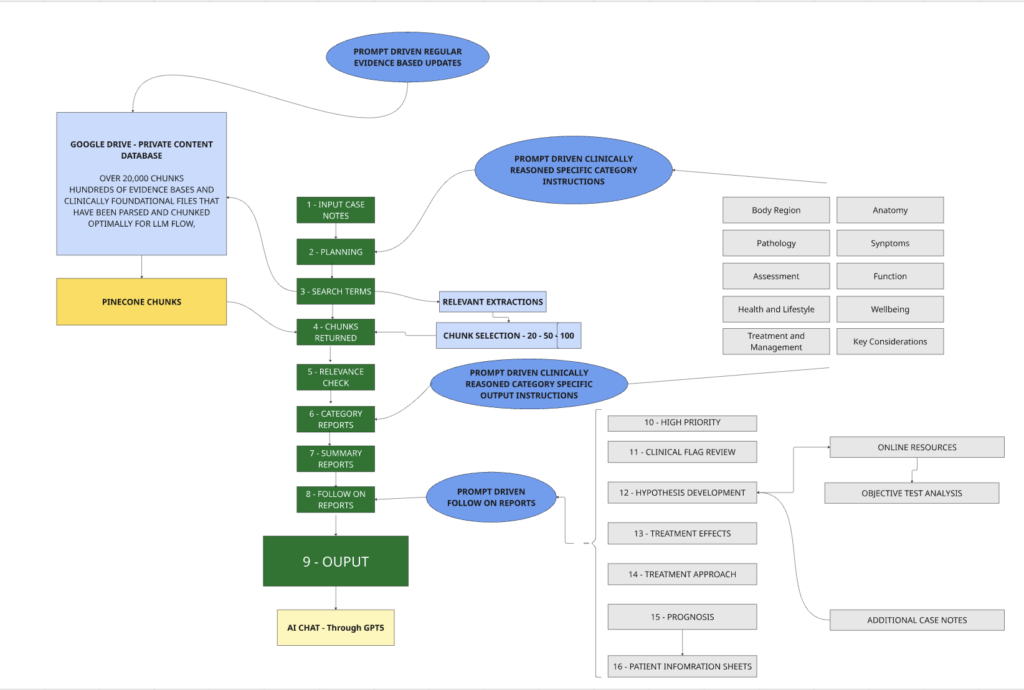
The Architecture
Physiotherapy isn’t a narrow diagnostic algorithm where symptoms in produces diagnosis out. It’s a reasoning practice grounded in anatomy, pathophysiology, clinical pattern recognition, and contextual judgment.
Restricting a resource like this to only high-quality RCT evidence would strip out much of what clinicians actually need:
Complex, layered presentations (which will never attract large RCTs)
Post-surgical rehabilitation protocols (difficult to randomise)
Manual therapy techniques (impossible to blind)
Neurodivergent presentations (under-represented in research samples)
Anatomical and pathophysiological relationships (that form the scaffold for all clinical reasoning)
The result would be a system that performs well on common, simple presentations but fails the moment a clinician encounters anything unusual or complex — precisely when AI support is most valuable.
Much of clinical practice rests on facts that are architectural rather than experimental: muscle function, segmental innervation, symptom patterns. These don’t need re-proving; what matters is recognising the associations and relationships between them.
So the 12,000+ knowledge chunks in this resource aren’t all “evidence-based” in the RCT sense. Many are. But more importantly, they’re all ‘clinically foundational’………
……….The Body Navigator combines this foundational knowledge with applied knowledge where an evidence base is required.